Why Understanding Anesthesia Regulations Matters for Healthcare Policy
Understanding TEFRA Rules, Billing Compliance, and Legal Risk


In anesthesia practice, care delivery models can include both anesthesiologists and CRNAs working together. However, the regulatory framework that governs how these clinicians collaborate and how services are billed can be confusing.
Terms like medical direction, medical supervision, TEFRA rules, and concurrency limits are frequently used interchangeably, even though they have very specific regulatory meanings tied to Medicare billing.
For educators, administrators, practicing clinicians, and legislators understanding the difference between billing rules, malpractice liability, and state regulatory standards is essential. Misunderstanding these distinctions can lead to compliance violations, accusations of fraudulent billing, or confusion about scope of practice.
This article breaks down the key differences.
Three Separate Systems Govern Anesthesia Practice
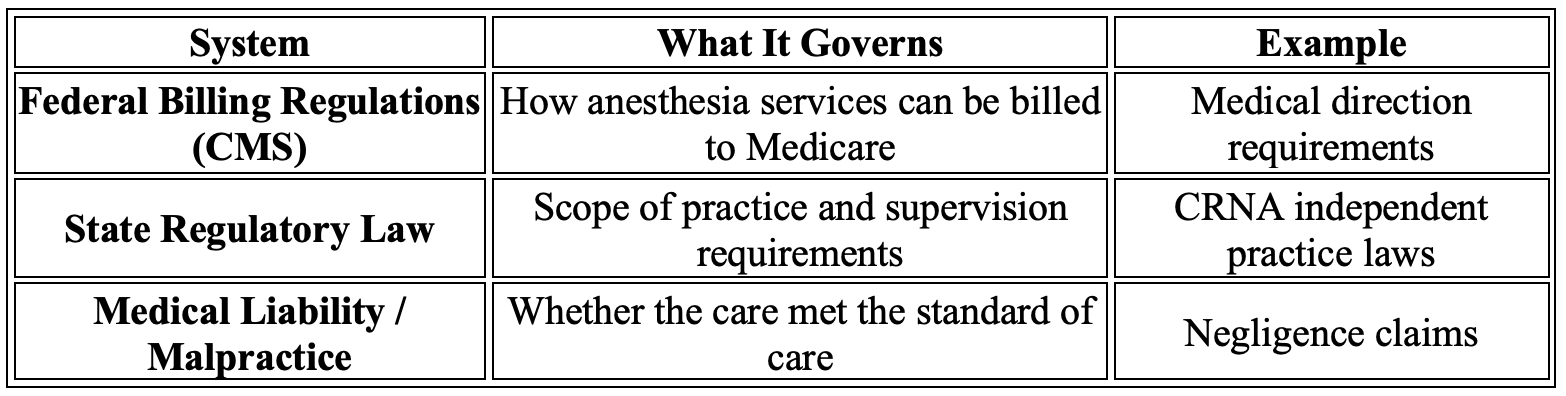
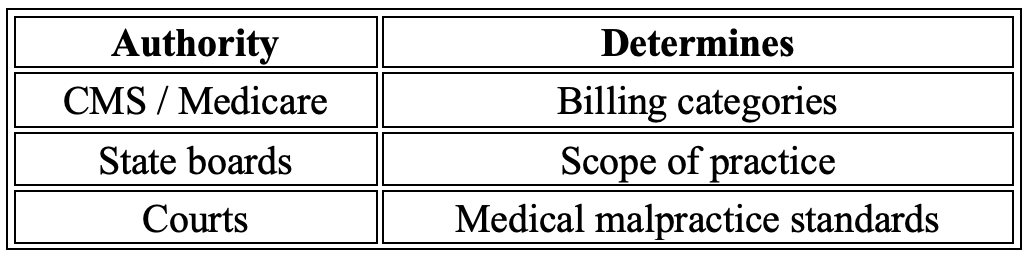
Anesthesia practice in the United States operates within three distinct regulatory frameworks that serve very different purposes:
• Federal reimbursement rules (Medicare billing regulations such as TEFRA)
• State scope-of-practice laws
• Hospital bylaws, DOPs and policies
These systems frequently overlap in practice but operate independently.
Medicare billing rules determine how anesthesia services are reimbursed. State laws determine who is legally authorized to provide anesthesia care. Hospital bylaws and policies as well as DOPs set what any provider can or cannot perform in that facility. The rule of thumb is the most restrictive of the 3 rules determines practice.
Confusion arises when these systems are treated as interchangeable. A practice model may be fully compliant with state law but violate Medicare billing requirements. Conversely, a case could meet all billing documentation standards yet violate the hospital policies, DOPS, and bylaws (if it says an MDA has to be there for extubation and they aren’t thats a violation regardless of state law or federal law).
Separating these frameworks helps clinicians, administrators, and policymakers better understand how anesthesia care is regulated in practice.
What is “Medical Direction”?
Medical direction refers to a specific Medicare billing category that allows an anesthesiologist to bill for services while directing CRNAs. This model is governed by TEFRA regulations, which require the anesthesiologist to personally perform or document specific elements of care.
Concurrency Limit
An anesthesiologist may medically direct up to four concurrent anesthesia cases.
If these requirements are met, billing and reimbursement for anesthesia services provided under medical direction:

The TEFRA Requirements
TEFRA refers to the Tax Equity and Fiscal Responsibility Act of 1982, which established the regulatory requirements for physician medical direction billing.
For a case to qualify as medical direction, the anesthesiologist must meet all seven TEFRA requirements:
Perform a pre-anesthetic examination and evaluation
Prescribe the anesthesia plan
Personally participate in the most demanding procedures
Ensure qualified anesthesia personnel are involved
Monitor the course of anesthesia at frequent intervals
Remain physically present and immediately available
Provide post-anesthesia care
Failure to meet any of these elements means the case may no longer qualify as medical direction billing.
What is “Medical Supervision”?
Medical supervision occurs when the anesthesiologist is involved with more than four concurrent cases or does not meet all seven TEFRA requirements.
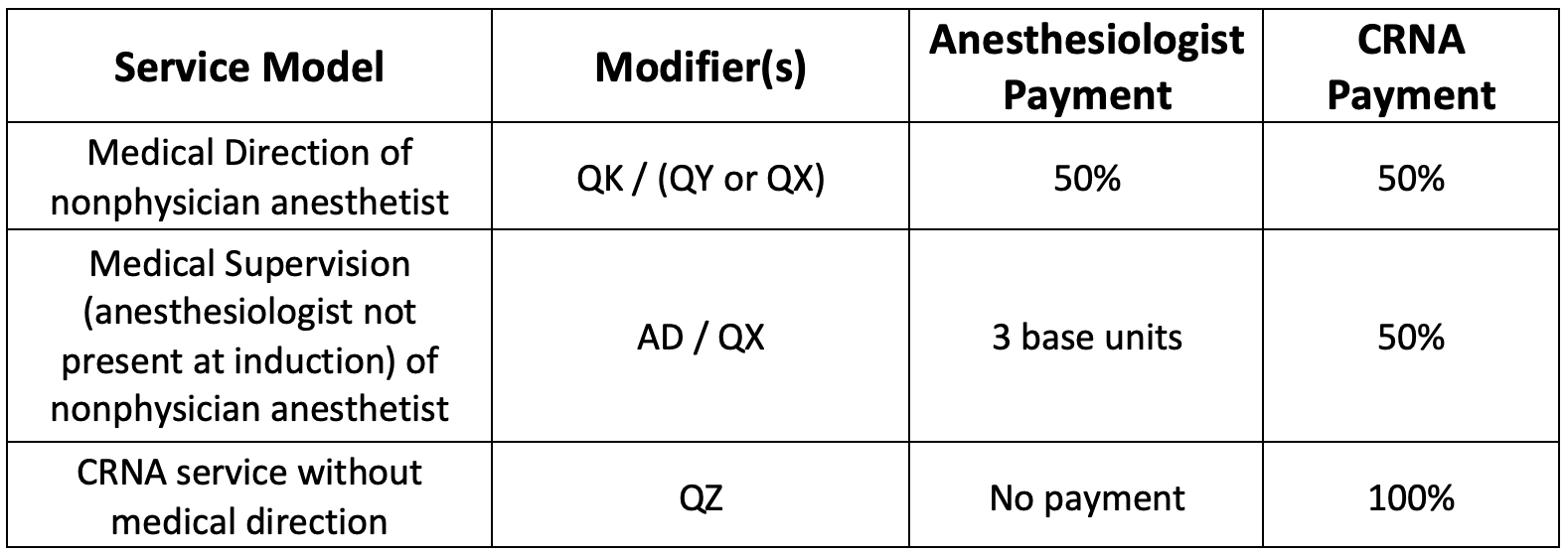
Under Medicare rules, medical supervision (modifier AD) represents a substantially reduced reimbursement category compared with medical direction. Under medical supervision, the physician anesthesiologist is generally limited to three base units per case and cannot bill anesthesia time units. In some circumstances a single additional "time unit" may be allowed if the physician is present for induction, but otherwise the physician side of the claim loses all time-based reimbursement. The CRNA can only bill 50% of the time units and 50% of the base units under QX billing. So "money is left on the table"
Billing and reimbursement for anesthesia services provided under medical supervision:

In this situation:
Medical supervision is therefore not equivalent to medical direction and does not require the TEFRA elements to be met.
Independent CRNA Practice
In many settings, CRNAs provide anesthesia care without physician direction.
This is billed using modifier QZ and the CRNA may receive up to 100% of the allowed fee.
Importantly, QZ billing does not imply reduced quality. It simply indicates that the service was not billed under the medical direction or medical supervision model.
Whether independent CRNA practice is allowed depends on state scope-of-practice laws and facility policies, not federal billing rules.
When Does Billing Become Fraudulent?
Billing fraud occurs when providers knowingly submit claims that misrepresent the service provided.
In anesthesia practice, common compliance risks include:
Documenting TEFRA steps that did not occur
If an anesthesiologist documents participation in key events but was not actually present, the claim may be considered false billing.
Improper concurrency documentation
If an anesthesiologist claims to medically direct four cases but was simultaneously covering more rooms, the claim may violate TEFRA requirements.
Copy-forward or template documentation
Documentation that automatically inserts required language without verifying the event actually occurred can also create compliance risk.
Fraud is fundamentally about misrepresentation in billing claims, not about clinical competence.
Fraudulent Billing vs. Medical Malpractice
A critical distinction exists between billing fraud and malpractice.

A provider could be fully compliant with TEFRA billing rules yet still commit malpractice if patient care falls below the standard of care.
Conversely, documentation errors in TEFRA billing could trigger fraud allegations even if the patient outcome was excellent.
Regulatory Compliance vs. State Practice Laws
Another common misunderstanding is assuming that Medicare billing rules determine scope of practice.
They do not.
TEFRA is strictly a billing regulation, not a clinical supervision requirement.
State laws determine whether CRNAs must be supervised, directed, or may practice independently.
For example:
This distinction explains why practice models vary widely across states and institutions.
How TEFRA Billing Structures Influence Anesthesia Workforce Economics
Another important consideration is how Medicare billing structures influence the economics of anesthesia care models.
Under the medical direction model, the total reimbursement for an anesthesia case does not increase when an anesthesiologist directs a CRNA. Instead, the payment for the case is divided between two providers, with the physician anesthesiologist typically billing 50% of the base and time units and the CRNA billing the remaining 50%.
From a reimbursement perspective, this means the medical direction framework primarily redistributes payment across multiple clinicians rather than increasing the total payment for the anesthesia service. In contrast, when anesthesia care is provided by a CRNA practicing independently and billed under modifier QZ, or an MDA independely billed under AA, the full reimbursement for the case is billed under a single provider claim. So the payment is the same but medical direction requires two providers to be paid and utilized instead of opening a second OR.
Understanding this distinction is important in workforce policy discussions, because billing structures can influence how anesthesia services are organized without necessarily reflecting differences in clinical capability or patient outcomes.
Why TEFRA Billing Rules Are Frequently Misinterpreted in Scope-of-Practice Debates
One of the most persistent misunderstandings in healthcare policy discussions is the belief that Medicare’s anesthesia billing rules establish clinical supervision requirements. They do not.
The TEFRA framework was created to define how anesthesia services are reimbursed when physicians and CRNAs work together. It determines when services qualify for medical direction billing and how payment is divided between providers. These rules are administrative and financial in nature. They do not determine who is legally authorized to deliver anesthesia care.
This distinction becomes particularly important in legislative discussions about anesthesia workforce policy. References to “supervision” in Medicare billing regulations are often interpreted as clinical supervision mandates, even though they function solely as billing categories. Whether CRNAs must practice under physician supervision is determined by state law and facility policy, not federal reimbursement rules.
Clarifying this distinction helps ensure that policy discussions are grounded in actual regulatory frameworks rather than misunderstandings of federal billing terminology.
Why This Matters for Educators and State Leaders
For nurse anesthesia educators and program leaders, understanding these differences is essential because graduates will encounter multiple anesthesia care models during their careers.
For legislators, understanding these distinctions is critical because policy decisions affecting anesthesia care should be based on clinical practice laws and patient safety evidence—not Medicare billing terminology. Clarity ensures that legislation accurately reflects how care is delivered and supports access to safe anesthesia services for their constituents.
Key takeaways include:
Medical direction/supervision is a billing structure, not a supervision law
TEFRA compliance is required for Medicare medical direction model reimbursement
Billing fraud relates to misrepresentation of services
Malpractice relates to patient harm and negligence
State laws ultimately determine CRNA practice authority
Confusing these concepts can lead to misinformed policy discussions, compliance errors, or unnecessary professional conflict.
Summary of anesthesia billing models:
Final Thoughts
The anesthesia care model in the United States operates at the intersection of clinical practice, federal billing policy, and state regulatory law.
Understanding the distinction between medical direction, medical supervision, TEFRA requirements, and malpractice standards allows clinicians and administrators to navigate this landscape more effectively.
Clarity on these issues helps prepare the next generation of anesthesia providers to practice both safely and compliantly in a complex healthcare system.
Clear understanding of the differences between billing regulations, scope of practice laws, and malpractice standards allows lawmakers to make informed policy decisions that accurately reflect how anesthesia care is delivered and ultimately serve the best interests of their constituents and the patients who rely on safe, accessible anesthesia services.
 | A guest post by
|
Excellent read! Thank you
Thank you for presenting this Substack.
Cost modeling for direction vs supervision is complex. Do you have a side by side example of a full day of OR cases billed under each model that shows the bottom line of reimbursement vs staff expense.
We have’s moved from supervision to direction and now incorporate AAs. I am curious if this actually improves the bottom line for the department.